


[ad_1]

Consider code descriptors, surgical anatomy, technology used, and type and amount of visualization.
Most CPT® codes get added to the code book each year without any mention as to whether the procedure is open or percutaneous, also known as minimally invasive surgery (MIS). Recently, the code development process is accounting for newer procedures that are supported by technologies that allow for a more streamlined and less invasive surgical approach. But misconceptions surrounding newer surgical approaches can throw a wrench in your coding. Make sure each of your providers is on the same page as you to ensure accurate coding.
The Difference Between Direct and Indirect
Confusion over appropriate coding of newer procedures performed as open or percutaneous is often due to interpretation of two accepted definitions of a surgeon’s visualization:
Direct visualization – Light-based visualization; can be performed by eye or with surgical loupes, microscope, or endoscope.
Indirect visualization – Image-guided (e.g., computerized tomography (CT) scan or fluoroscopy), not light-based visualization.
These definitions in the CPT® surgical guidelines may require additional review and context for coders interpreting many of today’s complex surgical procedures because:
- A surgeon’s light-based, performed-by-eye visualization of the anatomy in the operating room often does not tell the full story for coding professionals.
- Visualization alone does not settle the issue, as improvements in technology typically change the access and approach to many types of surgeries — and may change the coding solution altogether.
- Direct visualization does not always equate to an open procedure for coding purposes. In many cases, new technology allows for a procedure that may enable direct visualization of some of the surgical anatomy but is nevertheless MIS.
History: Endoscopic Spine Procedures and Direct Visualization
The advent of endoscopic spine technologies more than 20 years ago ushered in a myriad of procedures that may reduce surgical morbidity, as well as lower operative and patient recovery times associated with many common spinal procedures such as surgical decompression via discectomy or laminotomy. Endoscopic spine technology (a type of MIS) utilizes a combination of image-guided (scoped) work steps, alongside direct visualization of certain aspects of the surgical field via a narrow barrel, or cannula.
Many procedures were initially reported via an older open surgical decompression CPT® code, 63030 Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy, and/or excision of a herniated intervertebral disc; 1 interspace, lumbar. This code was originally added in 1993 for the open procedure types available at that time. Following the CPT® Editorial Panel’s review of endoscopic technologies, the descriptor for 63030 was changed in 2012 to specifically exclude the endoscopically assisted approach.
Despite arguments that endoscopic spine procedures could be appropriately reported via 63030 because they are sometimes assisted by directly visualizing (with the naked eye) a part of the surgical anatomy via cannula, the CPT® Editorial Panel ultimately declined to include the vignette within 63030 and instead created Category III codes to describe endoscopically assisted MIS spine procedures. CPT® code 62380 Endoscopic decompression of spinal cord, nerve root(s), including laminotomy, partial facetectomy, foraminotomy, discectomy, and/or excision of herniated intervertebral disc, 1 interspace, lumbar was added in 2017.
See Figure 1 for some of the more common considerations regarding appropriate CPT® coding of newer technology applied to existing procedures.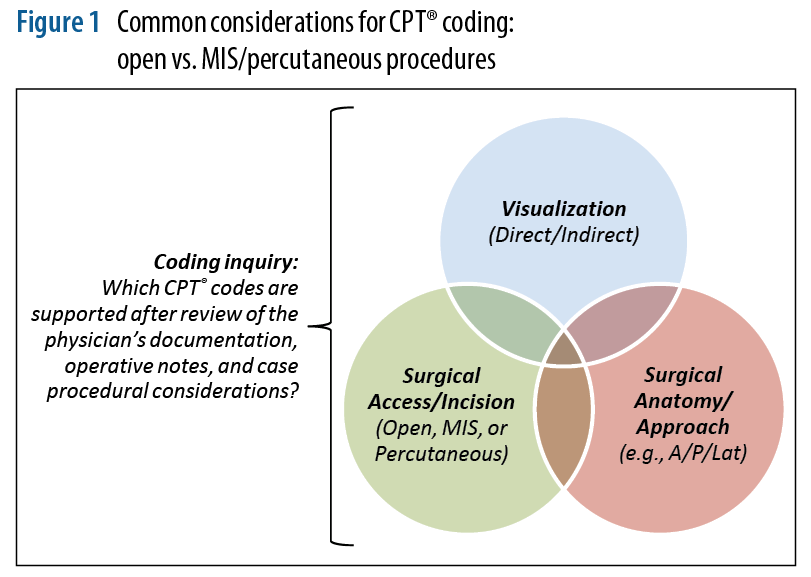
Case Study: MIS SI Joint Fusion
Coding experts interpret appropriate coding of spinal and orthopedic procedures based upon available definitions in the CPT® code book, including decision-making about direct visualization that draws from examples like endoscopic spine surgery. Coders also consider other case specifics such as incision size/length, surgical approach, duration of the procedure, and other operative details. Because technology and surgical advancements evolve faster than the codes, most orthopedic and spine code descriptors do not distinguish between open and percutaneous access. This discrepancy may lead to ambiguity and associated coding challenges.
One exception to this lag between technology and coding is a code added in 2015 to report lateral MIS sacroiliac (SI) joint fusion procedures using a transfixing device, placed “from the ilium through the sacroiliac joint to the lateral portion of the sacrum:” CPT® code 27279 Arthrodesis, sacroiliac joint, percutaneous or minimally invasive (indirect visualization), with image guidance, includes obtaining bone graft when performed, and placement of transfixing device. The CPT® Editorial Panel considered the new procedure different enough from existing SI joint fusion procedures performed via open incision and reported using 27280 Arthrodesis, sacroiliac joint (including obtaining graft). Concurrent with the adoption of 27279, the descriptor for 27280 was revised to more appropriately reflect the open incision and access utilized: Arthrodesis, open, sacroiliac joint, including obtaining bone graft, including instrumentation, when performed.
CPT® Assistant has provided guidance supporting the use of 27280 to report an SI joint fusion using an open approach requiring direct visualization. Vignettes associated with 27280 advise an incision length that runs “two-thirds of the iliac crest,” thereby allowing full, direct visualization of the SI joint.
Since that time, newer MIS procedures have emerged that use a posterior (dorsal) approach to the SI joint. This approach may allow for direct visualization of a part of the surgical anatomy. There is no open access to the joint with this MIS dorsal procedure, and only the lateral-most margin of the joint, where the two surfaces come together, is visualized. Due to the minimally invasive nature of the incision and the limited access to the articular joint surfaces, these procedures are not appropriately reported using 27280, which is intended to report an open procedure. The May 2021 CPT® Editorial Panel meeting proposed agenda includes an application for a Category III code to describe arthrodesis/stabilization of the sacroiliac joint via posterior or dorsal percutaneous or minimally invasive technique. The panel’s decision to clarify coding for this procedure type, distinguishing it from CPT® 27279 and CPT® 27280, may be helpful for coders and physicians. For the time being, use of an unlisted code, either for spine or hip/pelvis procedures, is more appropriate.
The vignettes associated with CPT® 27280 discuss an incision length estimated to be at least 8 cm or longer, based on typical SI joint anatomy, allowing full, direct visualization of all joint structures with the naked eye. Figure 2 provides a helpful analogy of a surgeon’s visualization of the SI joint in both open and MIS approaches using different configurations of two common dinner plates being held together at their edges.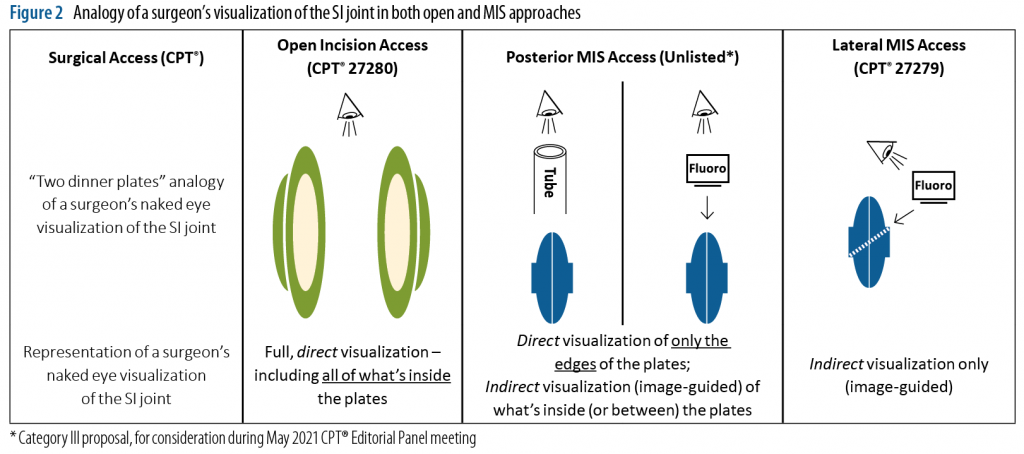
Based on a review of the relevant considerations and elements of visualization, access, and approach unique to each commonly reported type of SI joint procedure, the coding solutions shown in Figure 3 may be applied.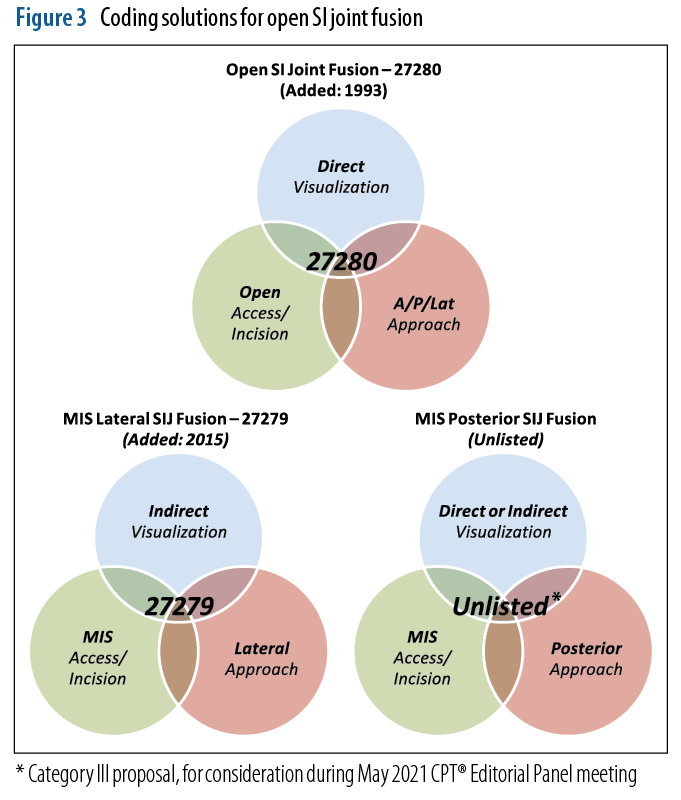
When in Doubt, Query
You may require additional information from the medical records before determining whether the direct visualization used in a procedure is appropriately reported via the open or percutaneous code. Some providers may choose 27280 when using a MIS approach based on the belief that any direct visualization is an open approach. When unsure of visualization or how much anatomy was viewed, it is appropriate to query the surgeon for this additional detail. It is important to be familiar with each approach and understand how they differ to ensure the provider documents the elements needed appropriately.
These examples of endoscopically assisted spine surgery and MIS SI joint fusion provide an excellent guide for how we should interpret direct visualization noted in operative reports, in lieu of existing codes for open versus percutaneous procedures.
Remember that new technology may affect the interpretation of existing codes by changing the visualization, surgical access, and approach taken. Consider asking clarifying questions the next time a provider asks you to apply an existing code to a new procedure.
If a provider is an early adopter of new technologies and performs MIS procedures in the future with greater frequency, have an upfront discussion about their expectations and their understanding of the potential coding solutions. In instances of newer technology use, an unlisted code may be used. Per Chapter 1 of the National Correct Coding Initiative Policy Manual for Medicare Services, “A physician should not report a CPT® code for a specific procedure if it does not accurately describe the service performed. An existing code should not be selected if it merely approximates the service provided.”
Resources:
https://www.joimax.com/en/company-history/
Butler, AJ, et al. Endoscopic Lumbar Surgery: The State of the Art in 2019.
Neurospine. 2019;16(1):15-23
https://doi.org/10.14245/ns.1938040.020
https://www.healio.com/news/orthopedics/20150116/approach-matters-how-the-type-of-spine-surgery-impacts-code-selection
Morningstar, M. CMS Issues Proposed Rule for 2021 Medicare Physician Fee Schedule: Specific Impact to Spine Procedures. Aug. 5, 2020. https://www.isass.org/proposedrule2021
AMA. CPT® Assistant. September 2013, Vol. 23, Issue 9
Lorio, MP. Editor’s Introduction: Update on Current Sacroiliac Joint Fusion Procedures: Implications for Appropriate Current Procedural Terminology Medical Coding. Int J Spine Surg Dec. 2020, 14 (6) 853-859; DOI: 10.14444/7136
https://finance.yahoo.com/news/tenon-medical-inc-releases-results-125800247.html
[ad_2]








{kind=link}